What is PEP?
PEP stands for Post-Exposure Prophylaxis and is a combination of drugs (usually lopinavir/ritonavir, emtricitabine and tenofovir) that will prevent replication of the HIV virus long enough for your body to clear it.
How does PEP work?
HIV PEP uses a three-pronged attack, aiming at elements of the virus essential for replication and that do not match processes used in human cells. This way the drugs attack the virus but do not interfere significantly in essential cell processes. It has three groups of drugs, a protease inhibitor (lopinavir/ritonavir), a reverse transcriptase inhibitor (emtricitabine) and a nucleoside reverse transcriptase inhibitor (tenofovir).
HIV is a retrovirus, which means it has an RNA rather than DNA genome. Before it can replicate in the cell it needs to change the RNA to DNA so that the human cell will recognise it and start making copies. To do this, it needs three things, the RNA genome as a template, a protein called a reverse transcriptase that reads the RNA and converts it to DNA and nucleosides/nucleotides (deoxyribose sugars) to make the DNA. The reverse transcriptase inhibitor binds directly to the viral reverse transcriptase preventing it from acting and stopping viral replication. The nucleoside reverse transcriptase inhibitor is a defective deoxyribose sugar that lacks the OH- group on the 3’ end. This prevents any deoxyribose sugar being added to the DNA strand after that point and stops the transcription dead.
The third prong of the attack is the protease inhibitor. If the virus gets past the reverse transcription inhibitors and makes viral DNA, the host cell will convert that DNA into a protein which is the functional element that the DNA is the plan for. This protein (gag-pol) needs to be cut in certain places to go from a pre-peptide to functional proteins. The protease inhibitor blocks the viral protease that cuts the pre-peptide, preventing the formation of functional virus particles. Working together these three elements effectively halt viral replication long enough for the body to clear the infection.
How effective is PEP?
PEP has been shown to clear the HIV from the system in >70% of cases. It is not a cure. It halts viral replication and so decreases the chances that an integration even will occur but will not undo any integration even that has already occurred. These events are very rare and are certain in non-treated HIV cases only due to the high number of virus and the time the body is exposed. The drugs can halt viral replication long enough for the immune system to recover and clear the virus. However, sometimes a recombination even occurs early in the infection and if this happens then the virus cannot be cleared. It is a bit like a game of Russian roulette, the longer you play, the more likely you are to get a bullet, but it can be in that first shot. This is why it is necessary to follow up after the PEP course to ensure the virus has been properly cleared. The only way to completely ensure you don’t get an HIV infection is to avoid contracting the virus in the first place. Practice safe sex with a partner who also practices safe sex.
What are the most common side effects of PEP?
- Headaches
- Backaches
- Dizziness
- Nausea
- Vomiting
- Diarrhoea
- Insomnia
- Depression
- Redistribution of body fat from the limbs to the torso
- Development of a buffalo hump
- Irregular heart beat
- Fainting.
That is not to say you will experience any or all of these, but they are normal to experience while taking this medication. Not all side effects will be listed on the information sheets. If you find you are experiencing a side effect that you can’t find a reference to does not mean it is not linked to the PEP or that you are imagining it. Only the most common side effects are listed as a rule. Anything you are unsure of please speak to your doctor.
What are the most serious side effects of PEP?
Liver damage seems to be the most common of the serious side effects. Jaundice, darkening of the urine and loss of appetite are the things to watch out for there. Kidney dysfunction is another thing to watch out for and you should speak to your doctor should you find significant changes to your toilet habits following PEP. Lactic acidosis is a rare but serious side effect where lactic acid builds up in the muscles (this is the substance that makes muscles ache after exercise). It can be fatal so seek urgent medical attention if you are suffering unexplained muscle aches, fatigue and dizziness.
One of the components of PEP can raise your blood sugar levels so it is important to keep a closer eye on those should you be diabetic. Those who are not diabetic should seek urgent medical attention should they find themselves exhibiting the symptoms of diabetes – increase thirst, increased urination, dizziness, fainting and fruity smelling breath.
Most of these side effects are rare but given that they can be fatal it is important to be aware of them and to seek emergency medical care should you suspect you are showing symptoms. A false alarm can be annoying, but it is better than ignoring valid warning signs. Make sure that you are having regular follow ups with your doctor during your PEP course, these are serious medications and can do real damage if not monitored correctly. If you have a good doctor, he or she will not mind you asking whatever questions you may have.
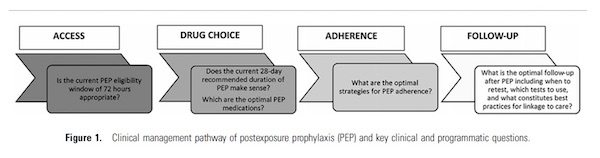
Do I need to take the full 28-day course?
Yes. The drugs to do not kill the virus, they stop it replicating. It is your own immune system that clears it and that has come under a significant attack by the HIV. You need to give it time to recover and clear the virus. There has been lots of research in this field and 28 days seems to give the best outcome.
Do I need to go to the same doctor for check ups?
No, but it is wise that you do so. HIV is a scary disease and the drugs to treat it are very strong, with side effects to match. A good relationship with your doctor can make a huge difference. It is easier to catch any problems if you are seeing the same person and they have all your previous data. Find a doctor you have confidence in and who you can ask questions of.
Can I take PEP if I am pregnant?
Yes, it is likely that PEP is safe if you are pregnant but it has not been proven that it is safe. Use only if absolutely necessary, but if you do have to use it, it is unlikely that the baby will be harmed.
Can I breast feed if I am on PEP?
No. All the PEP drugs have been found in breast milk so you will be giving them to your baby. You also run the risk of transmitting live HIV virus via the breastmilk. Baby milk formula is the safest choice in this situation.
What do I do if I forget a dose?
Take the dose when you remember unless you are within four hours of your next dose, then continue as normal. Do not take double the dose. It will not improve the effectiveness if you double up, but it will increase the severity of the side effects.
I have flu like symptoms when I take PEP, is this normal?
Yes. It is called Immune Reconstitution Syndrome and it is a result of your immune system recovering from the HIV attack. It is responding to threats that it was too weak to combat before the PEP treatment and is a good sign. If symptoms are serious, speak to your doctor.
Can I drink alcohol while taking PEP?
It is advised that you don’t. Alcohol is processed in the liver and all the PEP drugs can cause liver damage. Best to give it a rest for 28 days. That said, alcohol will not interfere with the activity of the drug and if you have half a glass at a special occasion it is unlikely to do any harm. Avoid binge drinking, your liver will thank you.
Can I have unprotected sex while on PEP?
No. The PEP drugs inhibit the virus, they don’t kill it. That is why you need to take them for a month. In most cases, your immune system is able to mop up the inhibited viruses before they can integrate into your genome and become chronic infections. Live virus is still present and while the chances of transmitting it are decreased, your blood and body fluids may still be infectious.
What Do We Do If Days Into Treatment, Another Exposure Occurs?
We added this answer based on a question from Quora.
Additional instances of exposure do happen with some degree of frequency. Both during, and immediately after HIV PEP treatment. On the one hand, people don’t always learn their lesson. On the other, there is the drive for sex, and the prevalence of drug abuse, particularly methamphetamine (ice), causing a decline in safe sex practices.
Going by the principle of the HIV PEP treatment protocol, a full 28 days of treatment should be completed after any potential exposure. Therefore, if a potential exposure did occur during treatment, then the end of the treatment should extend till 28 days after the point in time when the exposure happened.