Dental students in India aware of the risk of occupational HIV exposure and concept of PEP therapy but not aware of how to correctly use it
Continue readingKnowledge, Attitude and Practices toward PEP among Dental Students in India
Dental students in India aware of the risk of occupational HIV exposure and concept of PEP therapy but not aware of how to correctly use it
Continue reading
Several studies show evidence of the efficiency of Post exposure prophylaxis after sexual exposure to HIV (PEPSE) in preventing HIV.
Continue reading
Study finds evidence of reduced transmission risk behavior and reduced stimulant use in men who have sex with men through use of incentives
Continue reading
Knowledge on PEP among clinical medical students in developing countries is very low calling for inclusion of PEP in HIV curricula.
Continue reading
Availability of new integrase inhibitors offers better opportunities to improve efficiency of cART and PEP in controlling HIV replication.
Continue reading
Research has played a vital role in changing the face of the medical field. From untreatable diseases to highly contagious diseases, research made wondrous achievements and solved the previously unsolvable. The research on HIV has also provided us with life-saving treatments like a prophylaxis from HIV. The WHO (World Health Organization) convened a meeting in June 2014 to develop guidelines for the use of HIV post-exposure prophylaxis (PEP). During this meeting, gaps in research were also uncovered. This paper published in Clinical Infectious Diseases® reports the background, methodology, results and conclusions of a study to create a framework for future research.
The Grading of Assessment, Evidence, Development and Evaluation (GRADE) system and clinical management pathway were used for formulating the research questions required for future research. The study reported and analyzed current WHO recommendations for HIV PEP and graded its quality of evidence as well. The recommendations were formulated with the help of the Guideline Development Group (GDG) created by the WHO.
For the study, a clinical management pathway for HIV PEP was made which included the following steps:
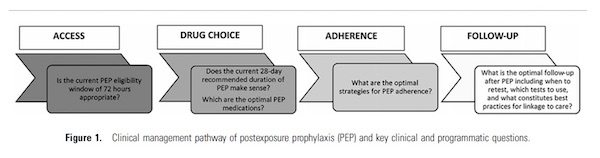
The formulated questions for each of the above mentioned clinical management pathway stage were thoroughly searched from current WHO guidelines and other online databases. The available data was collected, the gaps were identified and the GDG (Guidelines Development Group) helped the authors formulate future recommendations for each step.
Surprisingly, the study shows that the available guidelines of the WHO on the HIV PEP are mostly based on low-quality of evidence. Many of the clinical management questions that were formulated at the start of the study had no available study or recommendations.
On the whole, three study design formats for the future research were identified in the study which included the survey and interview driven research for identification of barriers related to PEP. Second was the establishment of a PEP registry on a global scale for drug choices, usage details, follow-ups and toxicities in specific drug regimen for PEP. Thirdly, randomized control trials for determination of the most authenticated evidence related to PEP.
For the study of access to PEP, the report suggests conducting cross sectional studies. To study the timing and duration of PEP, the recommendations are to have randomized control trials. These trials are also recommended for the study of the drug choice, adherence to the drug and the follow-up. Randomized control trials are lacking in comparing the HIV PEP drugs at different ages, hence the report recommends randomized control trials in it too.
The interesting thing reported in the study was that there is no future research needed in regard to the question whether a 28-day regimen for PEP is appropriate. The report mentioned that a 28 day PEP regimen is most appropriate and this recommendation does not need any future studies.
HIV PEP has been a revolutionary treatment that has prevented many who have been exposed to the HIV virus from getting infected. Information, news, scientific findings, views and recommendations have always been coming from healthcare institutions and scientific bodies, but seldom do we get the chance to know views and experiences of end-users who are prescribing PEP therapy. The views of the people using or have used post-exposure prophylaxis (PEP) were recently reported in a publication of the journal “Clinical Infectious Diseases”. This publication was developed by the WHO to help inform recommendations and guidelines for HIV PEP.
The study was conducted by gathering feedback and views from people using or have used PEP. Several methods were used in the study.
The results showed that the healthcare workers prefer the use and prescription of a 3-drug PEP based on the cost, availability and overall use. There was no significant difference in the opinion about the overall effectiveness of 2 versus 3-drug PEP.
When it came to online survey responses from healthcare workers with experience prescribing HIV PEP prescription to children, results were quite limited. From the results, there was a trend of using ritoinavir boosted lopinavir as the third drug in PEP when prescribing for children. while Efivirenz was preferred for children 3-10 years of age as the third drug.
Most of the healthcare workers were in favor of prescribing 28-day regimen for PEP. 65% of the respondents were of the opinion that besides HIV specialists, healthcare workers should be able to prescribe the 28-day PEP treatment. More than 86% of the health care workers believed that the Starter Pack is effective. 73% of the healthcare workers who were themselves using PEP preferred to be given 28-day PEP on their first visit.
Surprisingly, access to care was found to be the barrier for completion of PEP which included difficulties in access to the clinics and health care centers. The respondents emphasized that counseling plays a vital role in adherence to the PEP. The overall follow-up rate, knowledge of potential risks, and completion of PEP is better with counseling.
Although the data presented in this publication encompasses a variety of information but the quantity and quality of data is insufficient to help finalize PEP guidelines. As the information for the report was gathered from a limited population hence the authors believe that these results are not replicable to the general population.
Source:
The Human Immunodeficiency Virus (HIV) is not an adult-only disease but is also known to infect infants and children. The common causes of HIV infections in children are usually accidental needle stick injuries, premastication and sexual assault. Guidelines for adults recommend a base of tenofovir with lamivudine (3TC)/emtricitabine (FTC) and a third drug which is either a protease inhibitor or an integrase inhibitor. However, there is currently a lack of data to help form recommendations for age-appropriate HIV PEP formulations for children of different ages.
A recently published systemic review gathered the published data on the drugs and therapies used for HIV post-exposure prophylaxis (PEP) as well as ART for children living with HIV to make recommendations for the safe use of antiretroviral post-exposure prophylaxis in children. This study was conducted to help establish WHO guidelines on the choice of drugs to be used in PEP for children.
To prepare this report two different systemic reviews were conducted. In one of the works, published data was searched for studies which reported safety and completion rates of PEP in children. In the second review work, published data was searched for to find available evidence on the safety and efficacy of drugs used for antiretroviral medication therapy. The age group selected for the study were children at age 10 or younger – this age range was selected because children above 10 years old are usually given the same treatment as adults.
Completion Rates
For the first part of the study, out of total 97 studies screened initially, 3 prospective cohort studies were selected as per the selection criteria of the study. According to the reports, children in these studies (following injuries from needles in Canada and South Africa as well as sexual assault in Malawi) were given zidovudine and lamuvidine as part of a two-drug PEP therapy. This regimen had a completion rate of 64% in children receiving the medication for 28 days. The percentage of children who discontinued PEP due to adverse effects was 4.5%.
Efficacy and Risks
The second part of the study to evaluate the efficacy of drugs used as NRTI backbones, one randomized trial was identified to be included in the study. This paper compared abacavir with lamuvidine (3TC) and zidovidine with lamuvidine (3TC) and found that the regimen containing abacavir had better efficacy but the study reported one death and 1 treatment discontinuation due to hypersensitivity reaction.
3 studies were included to assess the choice of the third drug for children less than 3-year old. These studies compared lopinavir to nevirapine and found that there was a lesser risk of treatment discontinuation due to reactions when lopinavir was used. It was found that here was no difference in the efficacy of these drugs in children of age more than 3.
This paper concluded that a regimen of limuvidine, ziduvidine and lopinavir is recommended for a three-drug HIV PEP medication to be used on children. The medication should, however, be administered according to the weight of the children.
The alarming thing pointed out in the report is that there is very little published research related to drug efficacy, toxicity and usage in children affected or exposed to HIV. More studies are urgently required in this field so that better recommendations for the PEP of HIV in children can be formulated and tested.
Source:

With advancements in the field of research and scientific probing, we are continuously getting better treatments and vaccinations for different diseases. Although, there are currently no vaccines which can prevent HIV, scientists have been able to formulate the next best thing – HIV Pre-exposure Prophylaxis (PrEP). A report by the Center of Diseases, Control and Prevention compiled the recommendations and loopholes in the HIV research from published data on PrEP and HIV Post-exposure prophylaxis (PEP) to find a set of best practices for integrating these 2 highly effective HIV infection prevention methods.
Two effective regimens for the prophylaxis of HIV are PEP and PrEP. PEP is administered to individuals who have been exposed to HIV within 72 hours of exposure. Although, ziduvidine alone is effective in 80% of the time if administered within initial 72 hours, a 2-3 drug medication is recommended by the US Public Health Service in 2013. PrEP, on the other hand, is recommended for people who are living a high-risk sex life, even for those who are already on PEP and have been tested HIV negative. PrEP medication usually includes emtricitabine/tenofovir didoproxil fumarate and is effective in high-risk patients. In contrast, an early treatment regimen is offered as soon as the patient is found to be seropositive after exposure.
According to this report testing for HIV is still critical. HIV testing is recommended in all the cases especially when there is known or suspected exposure to HIV even when on a PrEP regimen.
The key element for the decision to start PrEP, PEP or early treatment after an exposure is dependent upon the antibody titer. Unfortunately, this test is not a good indicator for acute HIV infection where HIV RNA testing is recommended instead. The report says that HIV antibodies might not be detected using the antibody test during an early Acute HIV infection thus resulting in false assurances to the indivdual. This may lead to HIV-positive individuals starting on PrEP which may lead to drug resistance. A 4th generation test for HIV p24antigen can help if the test for HIV RNA is not available. This test has an advantage over 3rd generation and 2nd generation tests as it can detect HIV antibodies way earlier. Furthermore, the report suggests that the signs and symptoms can also guide the physician towards making a decision about acute HIV infection. Fever, myalgia, fatigue, skin rash and headache are common complaints in people with acute HIV infection.
According to the report, for individuals with a significant history of exposure, PrEP should be started even without the results of HIV testing. A single drug for PrEP and a three-drug regimen is recommended for PEP in US. After the completion of a HIV PEP regimen, it is recommended to start PrEP in people engaging in a high-risk sex life e.g. people with multiple sexual partners. The recommended test after 4 weeks of PEP is the 3rd or 4th generation HIV test as HIV RNS testing might be suppressed with a prophylactic treatment of HIV.
For PEP treatments, HIV testing is recommended at day 0, day 28 and 3 months after PEP. In the case of PrEP, testing is recommended at the start. Another test can be done after the first month on a PrEP treatment. Anyone on either PEP or PrEP treatment should be quickly started on early treatment if their blood shows seroconversion.
Source:
Grant M. R. and Smith K. D. Integrating antiretroviral strategies for HIV prevention: post- and pre-exposure prophylaxis, and early treatment. Open Forum Infectious Diseases Advance Access, 2015.
HIV holds a great threat to health care workers as constant exposure may lead to accidental HIV infection in previously un-infected individuals. A timely treatment of HIV Post-exposure Prophylaxis (PEP) is a prevention therapy that has been proven to be highly effective in protecting against occupational HIV infection. Due to its potential toxicities though, a substantial amount of people on PEP discontinue treatment. A study published in the BMC Public Health, in June 2015, reported the correlation of the adverse effects of PEP and the adherence to it. The study was conducted amount Health care Workers and Health care Students from the Korle-Bu Teaching Hospital, Ghana.
The cohort study was conducted on healthcare providers who were started with PEP due to HIV exposure from January 2005 till December 2010. A total of 228 exposed health care providers were included in the study. The risk assessment was done according to a preset in-house risk assessment system and with help with the guidelines set by the CDC. The medication was prescribed according to the risk exposure. The combination of lamuvidine/ziduvidine/lopinavir-ritonavir or lamuvidine/ziduvidine was administered in high-risk patients for 28 days. People with medium to low risk were given lamuvidine/ziduvidine for either 28 days or only for 3 days. The patients were followed up with blood analysis at week 6, month 3 and month 6 to check for sero-conversion.
Records of incidences of adverse reactions and adherence levels was maintained through telephone contact on day 3 and day 10 for the people who were prescribed the 3-day regimen. For people who were given a 28-day therapy, follow-ups were performed on day 3, day 10, day 20, day 28 and day 35 after the drug was dispensed.
Adverse reactions information related to the PEP treatment were collected from the participants with the help of a questionnaire. The adherence to the medication was assessed during the follow-up visit also with the help of a questionnaire.
The results were interesting to note as they showed that a total of 51% of the participants who received lamuvidine/ziduvidine for 3 days has a follow-up attendance of almost 65% compared to 90% attendance for those on the 28-day regimen. 52 out of 53 people who were receiving the three-drug medication of lamuvidine/ziduvidine/opinavir-ritonavir followed up. 16 people discontinued their two-drug PEP of lamuvidine/ziduvidine when they were found to be seronegative. Interestingly more than 80% of people reported that the time of their HIV exposure was less than 24 hours.
The highest adverse effects were reported to be with the three drugs PEP for 28 days followed by the two-drug PEP for 28 days. The least side effects were reported to be with lamuvidine/ziduvidine 3-day therapy. The most commonly reported side effect was nausea.
100% adherence to PEP was found with the 3-day lamuvidine/ziduvidine treatment. A significant decrease in adherence was noticed with the lamuvidine/ziduvidine treatment on the 28-day regimen (56 %) and the lamuvidine/ziduvidine/lopinavir-ritonavir combo treatment on the 28-day regimen (62%).
Source:
Tetteh R. A. et al. Adverse events and adherence to HIV post-exposure prophylaxis: a cohort study at the Korle-Bu teaching hospital in Accra, Ghana. BMC Public Health, 2015.